A report just published by the Department for Work and Pensions (DWP) further confirms high levels of trauma and mental distress among people not in employment and approaching benefits services for support. The report focuses on those in receipt of Employment and Support Allowance (ESA) aimed at people with an impairment or health condition that affects how much work they do.
VISION researcher Sally McManus, with colleagues Claire Lapham and Ann Conolly from the National Centre for Social Research, analysed the government’s main mental health study. They found that nearly one in three (30%) ESA recipients screened positive for post-traumatic stress disorder. This was more than twice the rate for Jobseeker’s Allowance (JSA) claimants (12%), and ten times that of employed people (3%). The analyses show that the claimant population experienced high levels of stress, in which self-confidence was low and anxiety high. Compared to those in employment, few ESA claimants owned their home and many faced serious debt arrears.
Sally presented findings from this study as oral evidence to the Work and Pensions Committee’s Inquiry into Safeguarding Vulnerable Claimants, including domestic violence victims. She drew attention to calls from Women’s Aid for reform they highlight is needed to make the benefits system the lifeline survivors need, rather than a source of re-traumatisation and further harm.
Women’s Aid recommendations include implementing a named domestic abuse lead in every Jobcentre Plus and ensuring staff receive regular, specialist domestic abuse training, so that work coaches and other frontline staff are better able to recognise claimants experiencing domestic abuse. Specialist domestic abuse services need to be properly funded to support and advocate for survivors in making their claims to DWP. Extending the domestic violence easement to up to a year would also help, alongside exempting those who are moving to or from refuges from repayment of Jobcentre Plus advances.
The definitions and methodology used in surveys to measure violence have implications for its estimated volume and gendered distribution. The Crime Survey for England and Wales (CSEW) uses quite a narrow definition of ‘violence against the person’ which excludes crimes which are arguably violent in nature.
VISION researchers Elouise Davies, Polina Obolenskaya, Brian Francis and Niels Blom worked with colleagues Jessica Phoenix, Merili Pullerits and Sylvia Walby to expand the CSEW’s measurement of violence to include threats, robbery, sexual violence and mixed violence/property crimes as violence.
The team investigates the implications of using an expanded definition of violence on the subsequent estimates of interpersonal violence and its distribution (the proportion of incidents of violence committed towards women, and the proportion of incidents that are committed by domestic relations rather than acquaintances or strangers). Additionally, they investigate how the expanded definition of violence shows an increased health burden of violence by investigating the number of injuries and the number and proportion of victims that are strongly emotionally impacted.
This results in a shift in the gender distribution of violence, with a higher proportion of violence against women (from 39% to 58%) and by domestic perpetrators (from 29% to 32%).
Impacts of violence – injuries and emotional harm – are also affected by the change in definition and disproportionally so for women.
However, much less is known about the effects of violence on the close relatives of victims. This is particularly surprising considering the critical role that relatives play in providing support, care, and advocating for victims in the aftermath of violence.
Cook, E. and McManus, S. (2024). Indirect victims of violence: mental health and the close relatives of serious assault victims in England. Social Science & Medicine.
The book’s chapters use retrospective case studies to engage with a systems approach to discover new thinking and applications that may best suit the area of domestic abuse and sexual violence (DASV). All the chapters showcase systems approaches in varying ways to ignite new inquiries and conversations about grappling with the greater complexity of problems.
Dr Adisa and Professor Bond, together with their collaborators, will launch the book at a special event at City St. George’s University of London on Tuesday, 26 November at 5.30 pm. They will explain the book and share their inspiration for the themes covered. A panel of speakers will share their collective vision for systems change in tackling DASV in different systems. The event will also feature poetry (spoken word) performances based on lived/living experiences of domestic abuse and as a survivor-centred response to the book’s themes.
Dr Adisa said:
“I am incredibly excited about the launch event. I have been overwhelmed by the positive and heartwarming reaction to the book from those committed to tackling the problem of DASV and those sadly affected by DASV. I have been impressed with the brilliant contributions made by all the authors who are deeply committed to bringing about change. This event is an opportunity to hear from some amazing speakers and forge new encounters and connections, united in our quest to reduce DASV and mitigate its devastating impact on children, families, and communities.”
Professor Sally McManus, Director of the Violence and Society Centre, and Co-Deputy Director, VISION, said:
“Dr Adisa works at the forefront of systems thinking. This new collection – co-curated with Prof Bond – brings a radical new approach to addressing violence and abuse, rooted in diverse real-world examples of challenge and change. The book houses many rich voices, distinct yet drawn together through common themes of complexity and hope.”
Please join Dr Adisa, Professor Bond, and their fellow collaborators at their 26 November book launch at The Pavilion, University Building, City St George’s, from 5:30 – 7 pm. Drinks and nibbles will be provided.
Adolescent domestic abuse (ADA) goes by many names, sometimes referred to as toxic teenage relationships. ADA includes physical, emotional, and/ or sexual abuse that occurs between young people who are, or were, dating. It is often overlooked in research, policy and practice. As a phenomenon, abusive behaviour between adolescents in intimate relationships remains relatively invisible, due in part to the persistent yet unfounded assumption that domestic abuse is something that only occurs between adults.
The Crime Survey for England and Wales finds that women aged 16 to 19 are more likely to experience domestic abuse than older age groups (ONS, 2020), but despite the prevalence, women in this age group are less likely to be referred to support services (SafeLives, 2017).
SafeLives discovered, on average, experiencing abusive behaviour from a partner begins at age 14 or 15, (2017). Further research in Wales found that among those aged 11-16 years old experienced a range of mental health and social impacts associated with experiencing domestic abuse, including teenage pregnancy, self-harm, and violent behaviour (Young et al, 2021).
With this landscape in mind and led by the need from our partners and to ensure intersectoral collaboration, VISION set up a working group with Thames Valley Police, SafeLives, Islington Borough Council, H.O.P.E Training, Respect, Youth Realities and others to investigate ADA via three activities:
ADA rapid systematicreview to synthesise existing research and data on ADA in teenage relationships (January 2024; funded by the City St George’s, UoL, Policy Support Fund).
ADA workshop: ‘Too Soon, Too Late’ organised by VISION with SafeLives Changemakers and young people who experienced abuse in their relationships when they were aged 13 to 16 (March 2024; funded by the City St George’s, UoL, Participatory Research Fund).
ADA conference, an event to bring together practitioners, people with lived experience, police, researchers, and policymakers working in the ADA environment (April 2024; funded by the City St George’s, UoL, HEIF KE Fund).
The report, Summary of the VISION Adolescent Domestic Abuse activities and events in 2024, is available online. It summarises the findings and recommendations of the review, workshop and conference for a roundtable of police, local government, academics, practitioners and specialist services working in the field held in June 2024. It was produced for the working group as an aid to distil the thinking thus far across the three VISION activities.
ADA Rapid Systematic Review
The VISION review investigates ADA by examining the terminology and related terminology used in the literature. The paper focuses on the perpetration and victimisation as it concerns adolescents, especially those under 16 years old, and the factors that act as protective and recovery mechanisms for young people experiencing ADA.
VISION researchers, led by Dr Ruth Weir, conducted a systematic rapid review of 79 papers from databases for peer-reviewed literature.
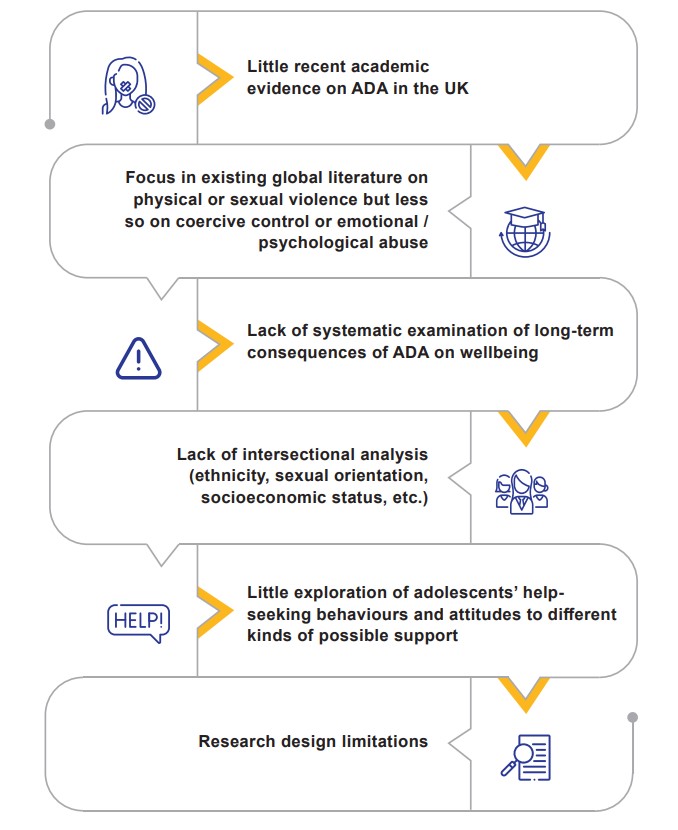
The team discovered definitional issues, an overemphasis on quantitative studies, and a lack of attention to ADA when it intersects with cultural factors, gender differences, criminalisation, and poor mental health. Many of the studies report on school-based settings, with limited reporting and understanding of the role of neighbourhood factors in acting as protective and recovery mechanisms. Additionally, literature on impacted adolescents and their help-seeking behaviours is sparse. The review revealed that evidence on abuse affecting adolescents in the UK remains patchy.
Highlights from the VISION ADA rapid review: Gaps, limitations & considerations for future research
ADA workshop:Too Soon, Too Late
Dr Polina Obolenskaya and Dr Annie Bunce, VISION Research Fellows, collaborated on a consultation project, “Too soon, too late”, with the SafeLives Changemakers and with young people who experienced abuse in their relationships when they were aged 13 to 16. The main aim of the consultation was to develop a robust, methodological framework for a future adolescent domestic abuse (ADA) research proposal.
Together with SafeLives, a charity working to end domestic violence, they co-developed the material for the online workshop, a focus group, with young people, which took place in March 2024, and was facilitated by the ‘Changemakers’, a group of young people passionate about amplifying the voices of survivors of domestic abuse. They work alongside SafeLives providing a young person’s expertise on the charity’s work, conducting research, and working to influence policy change.
Some of the preliminary themes from the workshop include:
Lack of recognition amongst young people of both domestic abuse (DA) in general, and ADA specifically.
Young people don’t easily identify their own experiences of ADA as DA.
Young people’s understanding of ADA changes over time.
Young people highlighted the wide variation in experiences of ADA and professional responses to it.
Young people can identify clear priorities for future ADA research.
Young people see school as a key point of early intervention, but feel that improvement is needed in terms of better education around healthy relationships and school cultures that encourage open discussion around DA whilst actively challenging attitudes and behaviours conducive to ADA and sexual violence.
Further information can be found in the report available for downloading online.
ADA Conference
The Adolescent Domestic Abuse conference held on 18 April brought together 161 academics, practitioners, and policy makers to share existing research, policy and practice. Dr Ruth Weir, Senior Research Fellow at the Violence & Society Centre and the VISION research project at City, and Katy Barrow Grint, Assistant Chief Constable at Thames Valley Police, welcomed the delegates.
Louise Rolfe, OBE, Metropolitan Police and National Police Chief Council lead for Domestic Abuse was a keynote speaker. Louise spoke about the national context of domestic abuse, highlighting the most harmful abuse that is seen is coercive control and that domestic abuse accounts for more than 30% of violent crime. She also spoke about the role of the media requiring scrutiny and the need for sustainable long-term systemic solutions.
Professor Christine Barter, Co-Director of the Connect Centre for International Research on Interpersonal Violence and Harm, University of Central Lancashire, also gave a keynote. She provided an overview of her 15 years of research exploring the prevalence, subjective impact and risk factors associated with abuse in young people’s relationships in her presentation, Researching abuse within teenage relationships: A critique of a decade’s work and what we could do better. Her mixed-method body of work addressed both victimisation and perpetration for young people aged 13 to 17.
There were panels on Teenage relationships and abuse: What the research says; Sexual violence in teenage relationships; and Specialist services and local government. Presenters included academics sharing their ADA research from Loughborough University and Durham University and specialist domestic violence organisations like SafeLives, Refuge, and Women’s Aid. Islington Borough Council, representing local government, discussed their work on a multi-agency model project to identify, intervene and protect teenagers experience ADA.
Workplace bullying and harassment (WBH) is bad for people’s health, and this negative health impact can manifest in a variety of ways and be long-lasting.
Over a decade ago the UK government initiated the Fair Treatment at Work survey, aiming to ‘place the issue of bullying at work on employers’ agendas’, yet there has been no major initiative since.
Using data from the 2014 Adult Psychiatric Morbidity Survey, VISION researchers Annie Bunce, Ladan Hashemi and Sally McManus, along with Carrie Myers and Charlotte Clark from City St George’s, University of London and Stephen Stansfeld from Queen Mary, University of London, examined the prevalence and nature of WBH among workers in England, and associations with mental health.
A clear picture of the severity of the problem of WBH in England is painted by four key findings.
One in ten people in paid work reported having experienced WBH in the past year. This is likely to be an underestimate due to underreporting for various reasons;
Those who reported bullying were more likely to be in a financially disadvantaged position;
Over half of people who reported having been bullied at work identified the perpetrator as a line manager; and
Clinically diagnosed common mental disorder was more than twice as likely in employees with experience of WBH compared with those without, and those exposed to WBH were also twice as likely as others in paid work to screen positive for PTSD.
Taken together these findings demonstrate that WBH is common in UK workplaces, it may be driven and exacerbated by issues of inequality, power and hierarchical organisational structures, and it is associated with depressive and anxiety disorders severe enough to warrant health service intervention and treatment.
This power dynamic should not be forgotten when addressing issues in the workplace, but the complexity of workplace environments creates challenges for identifying, understanding and addressing bullying. Reports of WBH can coincide with performance concerns from managers, and, whilst behaviours intended as legitimate performance management activities might be misinterpreted as bullying by the employee, it is also possible that HR practitioners attribute managerial bullying behaviours to legitimate performance management practice to exonerate mangers and protect the organisation.
This links to a recently published piece for The Conversation by Sally McManus and Kat Ford (Bangor University), which sets out how companies can influence and perpetuate violence in society, including via employment practices that conceal the extent of bullying, sexual harassment and other forms of workplace violence (for further information see Six ways companies fuel violence (theconversation.com).
Also, structural issues in the workplace can create pressure for managers which they then take out on those they manage, managers can be victims of WBH themselves, and organisational culture may perpetuate WBH.
Given such complex power dynamics, it is recommended that organisations involve employees at all levels in the development of policies, and collaboratively review the implementation and performance of policies regularly to ensure they are working for the people they are intended to protect. Rather than prescribed ‘tick box’ policies and responses, creative methods incorporating employees’ perspectives may more likely lead to meaningful change.
VISION seeks to highlight the wider contexts in which violence occurs. To tackle the causes of violence and improve violence reduction strategies, governments tend to look to families, communities, schools, health and justice services, and community and voluntary sector organisations for solutions. While these are crucial, a broader and more radical approach is also needed.
For decades, health researchers have raised awareness of various ‘commercial determinants of health’. Initially, this work focused on industries producing harmful products like tobacco, alcohol, fast food and fossil fuels. However, the approach has expanded to show how a much wider range of companies and industries harm our health through their various practices.
We applied an existing framework to unpack the specific ways in which companies and commercial processes might shape not only our health – but also the nature and extent of violence in societies. The analysis was carried out by Kat Ford from the Public Health Collaborating Unit at Bangor University, Karen Hughes from Policy and International Health, World Health Organization Collaborating Centre on Investment for Health and Wellbeing, Public Health Wales, and VISION researchers Mark Bellis, Olumide Adisa and Sally McManus.
A summary of six of the ways in which companies can fuel violence has been published in The Conversation. They include political practices like lobbying against safety legislation, and financial practices like investing in regimes with poor human rights records. The full paper details these and other commercial processes and argues that governments need to consider the role and influence of companies if violence prevention is to be effective.
By Dr Alexandria (Andri) Innes, VISION researcher and Senior Lecturer in International Politics at City, UoL
This research makes a case for shifting how we use and think about securitization theory. Securitization theory conventionally offers some insight into how certain issues are brought under the umbrella of security – normally state security – rather than sitting in normal political debate. When something is securitized more extreme or authoritarian policies that would normally be controversial in liberal democracies can be used. This might include things like removing civil liberties such as freedom of speech or freedom of assembly, or indefinite detention, or even policies that we’re all familiar with from 2020 and 2021, prohibiting freedom of association and freedom of movement in public space.
Securitization theory has focused on process (how something becomes securitized), object (what is securitized), and subject (who is being protected). The latter is generally the state and/or society. The process works through a meaningful speech act suggesting something is a security issue or framing it in security language (think about the war on drugs or the war on terror). The speech act then has to be accepted by an audience, who might be society at large, or the public, but also might be specialist practitioners, policy makers, think tanks, civil society, educators and so on. And the object of securitization is anything where this type of totalising discourse is evident. Examples include health, transnational crime, climate change, religion, humanitarianism, terrorism, particular ethnic identities, and immigration along with plenty of other things.
In this article, I argue that we should consider inequality when deconstructing and attempting to understand the process and practice of securitization. I suggest that racialization, ethnicization, and gendering create structural inequality in the ordering of what we think of as international – a world composed of equal state units. The nation state relies on these processes to function as an identity unit in the way that it does (with passport carrying, rights-bearing citizens and the right to deny rights to people who are not in the correct in-group). I propose that securitization theory might do better at dealing with inequality of we focus on the experience of being securitized, more so than the speech acts that make that securitization happen.
The article functioned more as a review of this sub-paradigm, and turns attention to the way the ‘object’ part tends to be siloed into the relevant thematic areas. So we look to just one securitized object at a time. Here, the article looks instead at three processes of securitization, to show that the siloing means the forms of inequality inherent in the nation state and national security are reproduced rather than reckoned with.
I look at the securitization of health, the securitization of immigration, and the securitization of gender-based violence. I suggest by mapping these objects of securitization together, we can better see the intersectional violence of inequality played out, and make visible the vulnerability, inequality and violence that pre-exists securitization, but is also enhanced, aggravated and at times hidden by it.
Social media platforms enable people to communicate in both positive and negative ways, including in ways that may be abusive and bullying. Abusive messaging can harm mental health, and has been shown to increase during periods of public crisis, such the Covid pandemic. There is a need to better identify and classify cyberbullying and online abuse, to improve the design of deterrence strategies.
In a recently published study VISION researcher Dr Lifang Li explored how the ‘verification status’ of social media user accounts was associated with cyberbullying. Verification refers to when a social media user’s identity has been confirmed, for example by the checking of an identity card. Lifang examined data from China’s main social media platform, Weibo, to classify messages that had been posted during the pandemic about people who were diagnosed with the coronavirus. She examined the content of posts made by users who were verified and unverified, used techniques to understand how often anger-related words were used, and measured the extent to which the posts got shared.
Posts that could be classified as critical of people diagnosed with Covid during the pandemic (for example, describing them as ‘reckless’ or ‘selfish’ for having contracted the infection) were in the minority, most social media users were understanding or neutral in their online communications. Lifang found that posts that were critical of people diagnosed with Covid were more likely to use anger-related words. Although not a focus of the paper, official verification of a social media user’s identity did not appear to be strongly related to how likely they were to post or repost critical views.
However, male verified social media users were more likely than unverified or female users to have their posts shared. This suggests that their online activity may have a disproportionate impact on other users. Cyberbullying monitoring may need to consider such differences, especially in the context of public health crises.
This study made novel use of machine learning techniques, which may help other researchers developing algorithms to identify abusive posts online.
The question of how we measure, categorise, and represent ethnicity poses a growing challenge for identifying and addressing ethnic inequalities. Conceptual critiques and qualitative studies highlight the complexities and challenges of measuring ethnicity, yet there remains a lack of quantitative studies investigating the implications of these complexities for inequalities research.
VISION researchers, Hannah Manzur, Niels Blom, and Estela Capelas Barbosa, address this gap by scrutinizing methodological processes and analysing the implications of measurement and categorisation in the Crime Survey for England and Wales (CSEW), critiquing the UK’s standardised measurement of ethnicity in national survey data and government statistics.
Based on their comparative quantitative analysis of standardised ethnicity categories and regional origins and their evaluation of the CSEW and census’ methodologies, they propose an alternative categorisation of ethnicity, focusing on the ‘Mixed’, ‘Asian’, and ‘Latinx/Hispanic’ ethnic groups.
Using adjusted crosstabulations and logistic regression models, they found variations in ethnic patterns of violence victimisation based on standardised measures and their alternative recategorisation, particularly relating to the distinction between ‘Asian’ sub-groups, the recategorisation of ‘Mixed’ ethnicities, and the inclusion of ‘Latinx/Hispanic’ as a distinctive ethnic group.
Their findings reveal valuable insights into the implications of ethnic categorisation for understanding violence inequalities, with significant implications for further policy and research areas.